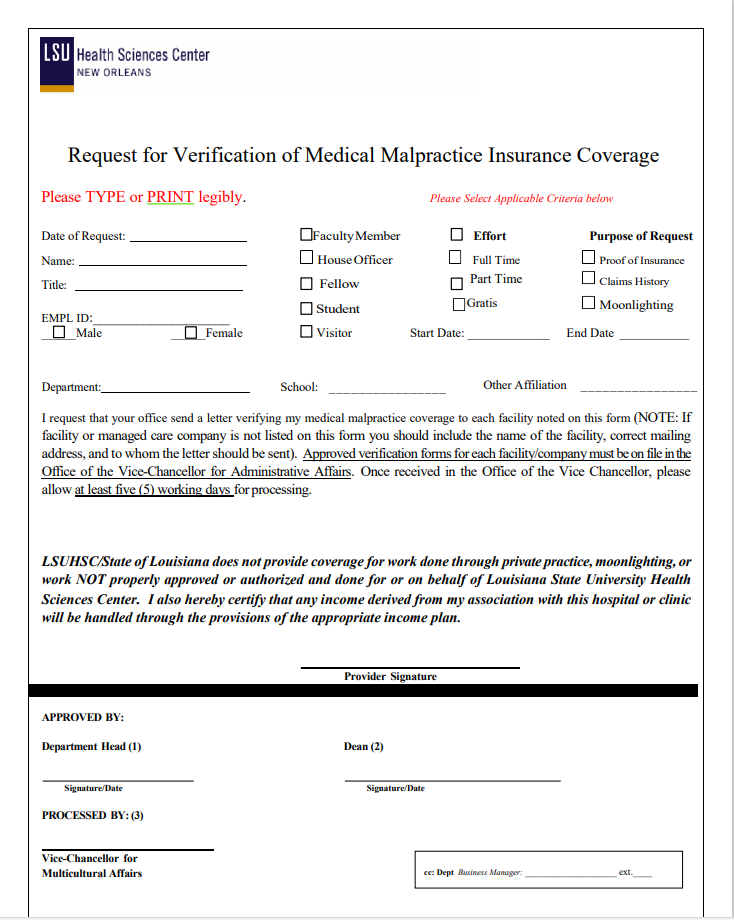
Print the Malpractice Spreadsheet, attach to this form, and submit to the GME office for GME signature. Once processed in GME, it will be sent to the Vice Chancellor's office. When filling out the Malpractice Form, only 1 copy of the form needs to be filled out and submitted. Under the "Name" and "Title" fields in the form, put "See Attached" as the spreadsheet will have all of the needed information for each resident.
Requester should contact Cynthia Scott directly.
| Filter by label (Content by label) |
|---|
| showLabels | false |
|---|
| title | Places This Form is Referenced |
|---|
| excerptType | simple |
|---|
| cql | label = "malpractice_form" |
|---|
|